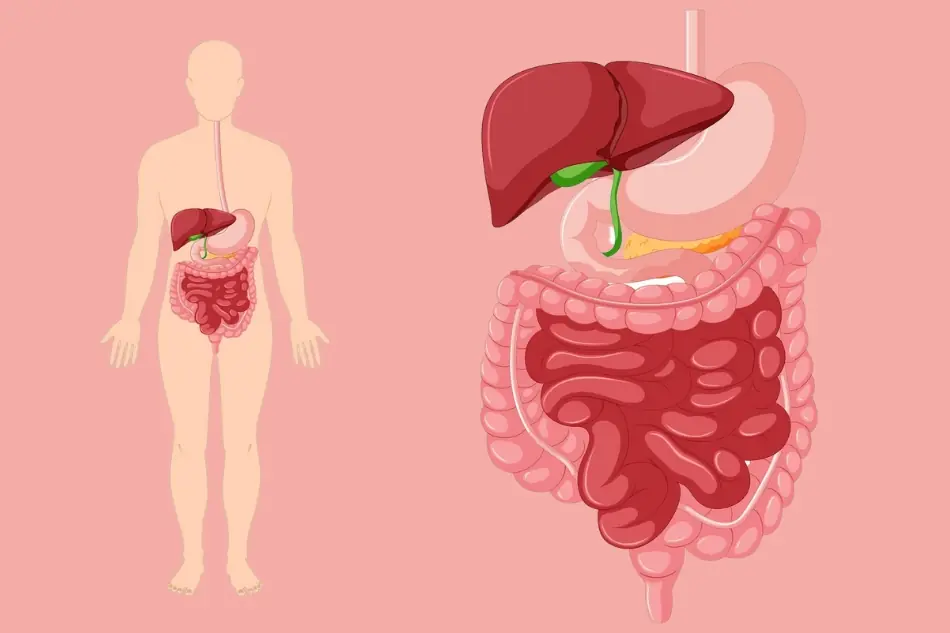

What Your Feet May Reveal About Your Liver Health: 15 Signs to Know
15 Foot Clues That Could Indicate an Underlying Liver Issue
⏱️ 1 min read 11/08/2026 17:18
15 Foot Clues That Could Indicate an Underlying Liver Issue
They never imagined he was the officer evaluating their character all along.
Winged Beans: The Overlooked Vegetable With Impressive Nutritional Benefits
Eating More Rice Than You Need? These Effects May Surprise You
Bubble Wrap Isn’t Just for Packing: Try This Clever Kitchen Hack
Do You Experience These 3 Symptoms at Night? Learn When They May Be a Cause for Concern
5 Morning Habits That May Affect Bl00d Pressure and Cholesterol
Avocados Are a Favorite Superfood—But Their Effects on Your Body May Surprise You
Kidney Health Alert: 5 Vegetables You May Need to Limit in Certain Conditions
2 Tablespoons a Day? Here’s How It May Support Your Digestion
Got a Sebaceous Cyst? Here’s What You Should Know
The Missing Bride and the Stranger in White
Severe Constipation and Toxic Megacolon: What You Need to Know
The Truth Before the Wedding