Most Drivers Have No Idea What the Tiny Button on a Seat Belt Is Actually For
A small seat belt part plays a bigger role than most people realize.
⏱️ 1 min read 11/08/2026 22:50
A small seat belt part plays a bigger role than most people realize.
Seeing Coarse Hair on Your Chin? Don’t Ignore the Change—Here’s What You Should Know.
Hidden Parasites in Your Food? Doctors Warn About These 4 Common Foods.
Why Do Dogs Sniff People’s Private Areas? The Science Behind This Common Behavior May Surprise You.
My Grandma’s Finger Joints Started Looking Knobby—Then More Bumps Appeared. What Could Be Behind It?
Dreams of lost loved ones often carry deep emotions and meaning.
Your Legs Cramp While You Sleep? ⚠️ Here’s What Specialists Say You Should Pay Attention To.
White Spots on Your Skin? Before You Worry, Here’s What Experts Say They Could Mean… Check the 1st Comment 👀
A handful of walnuts daily may support heart, brain, and gut health.
A simple breakfast habit may support energy, fullness, and health.
Most People Miss These 10 Nighttime Signs of Diabetes
Your ideal type may reveal hidden traits and preferences within you.
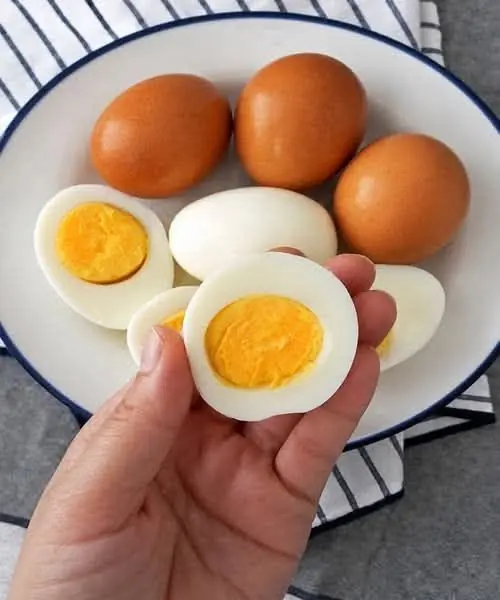
A high-egg diet brought unexpected health changes after five months.
A simple eggshell trick is helping gardeners protect plants naturally.
Don't Ignore These 12 Warning Signs Women Should Know