Oa Oa fish, also known as the giant salamander or giant newt, is a rare and fascinating species of amphibian found in China and Japan. This creature, scientifically named Andrias davidianus, is the largest amphibian in the world. It typically lives in mountain streams or lakes in China and Japan. Currently, this species is at risk of extinction due to environmental pollution and over-hunting by humans. The Oa Oa fish is primarily found in the Yangtze River and the Yellow River.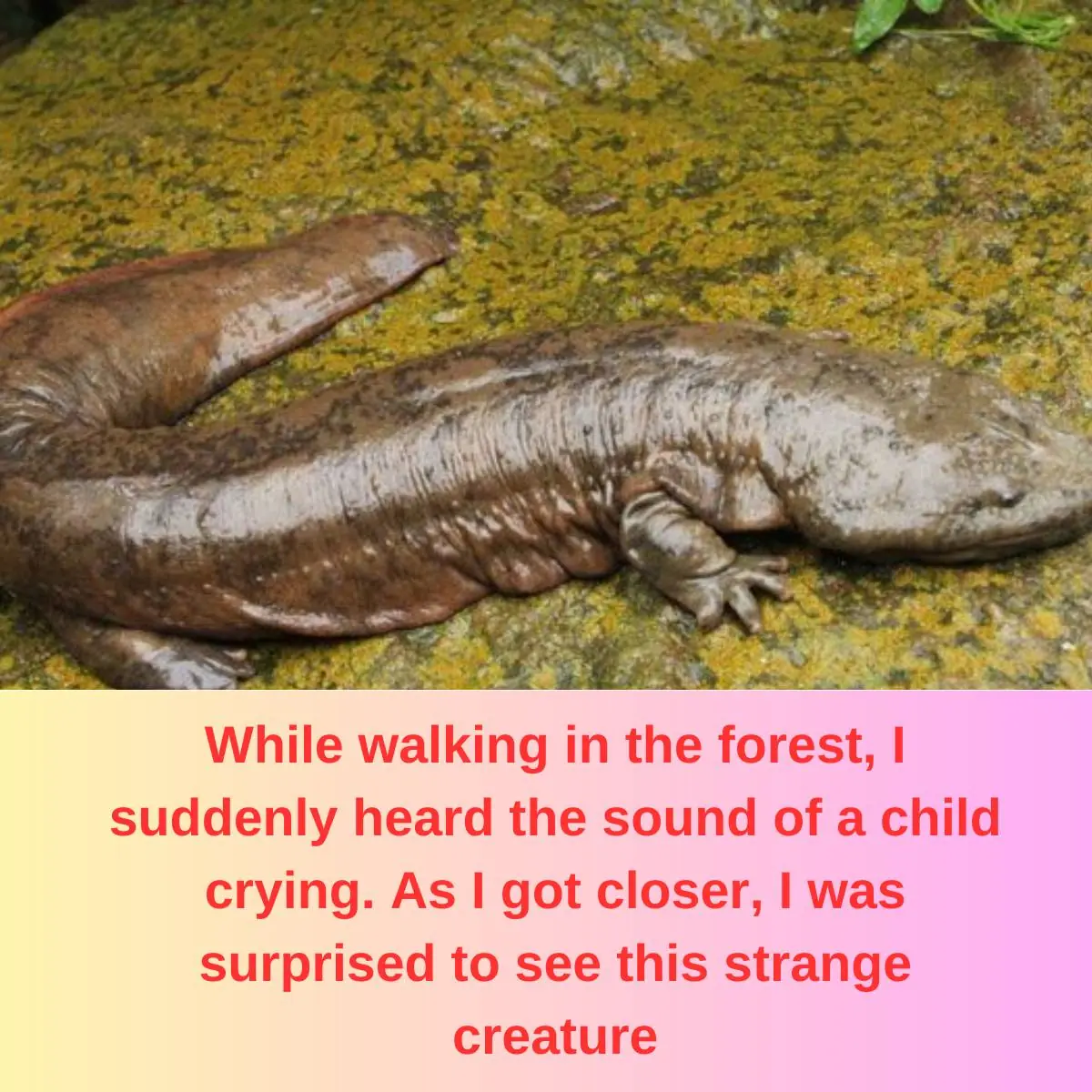
The Oa Oa fish has a distinctive cry that sounds like a child crying, which often causes fear among those who hear it, especially during quiet nights. This unique sound has led to the fish being nicknamed "Baby Fish," "Child Fish," or "Oa Oa Fish" in some places. These creatures grow to a size of 120 cm to 180 cm, weigh up to 50 kg, and have a long lifespan. Some Oa Oa fish have been discovered to live for up to 200 years in limestone caves in southwestern China.