Discover 5 Ways Watermelon Seeds Can Boost Your Health
5 Health Benefits of Eating Watermelon Seeds
Garden 31/03/2026 22:43

Cantaloupe, known for its sweet, juicy flesh and vibrant orange color, is a favorite summer fruit. Whether you're growing it for its delicious flavor or simply for the joy of cultivating something from scratch, cantaloupe can be an incredibly rewarding crop to grow in your garden. This guide will walk you through the essential steps of cultivating cantaloupe, from choosing the right variety to harvesting your fruit.
Cantaloupe belongs to the Cucurbitaceae family and is closely related to melons like watermelon and honeydew. There are different varieties of cantaloupe, and selecting the right one for your climate and growing space is important. Popular varieties include:
Galia: A small, round melon with green flesh and a sweet taste.
Cantaloupe (Muskmelon): The classic orange-fleshed melon most commonly found in supermarkets.
Sugar Cube: A smaller melon, perfect for limited spaces and offering a high sugar content.
When choosing a variety, make sure it is suitable for your growing zone. Cantaloupes require a warm growing season with temperatures between 70-90°F (21-32°C).
Cantaloupes thrive in well-drained, sandy-loam soil that is rich in organic matter. Here’s how to prepare the soil for planting:
Location: Choose a sunny spot in your garden where the plants will get at least 8 hours of direct sunlight per day.
Soil Preparation: Cantaloupes prefer slightly acidic to neutral soil with a pH of 6.0 to 6.5. Amend your soil with compost or organic matter to improve fertility and drainage.
Soil Drainage: Ensure the area is well-drained to prevent root rot. If your soil is clayey or compacted, consider creating raised beds or mounds to improve drainage.
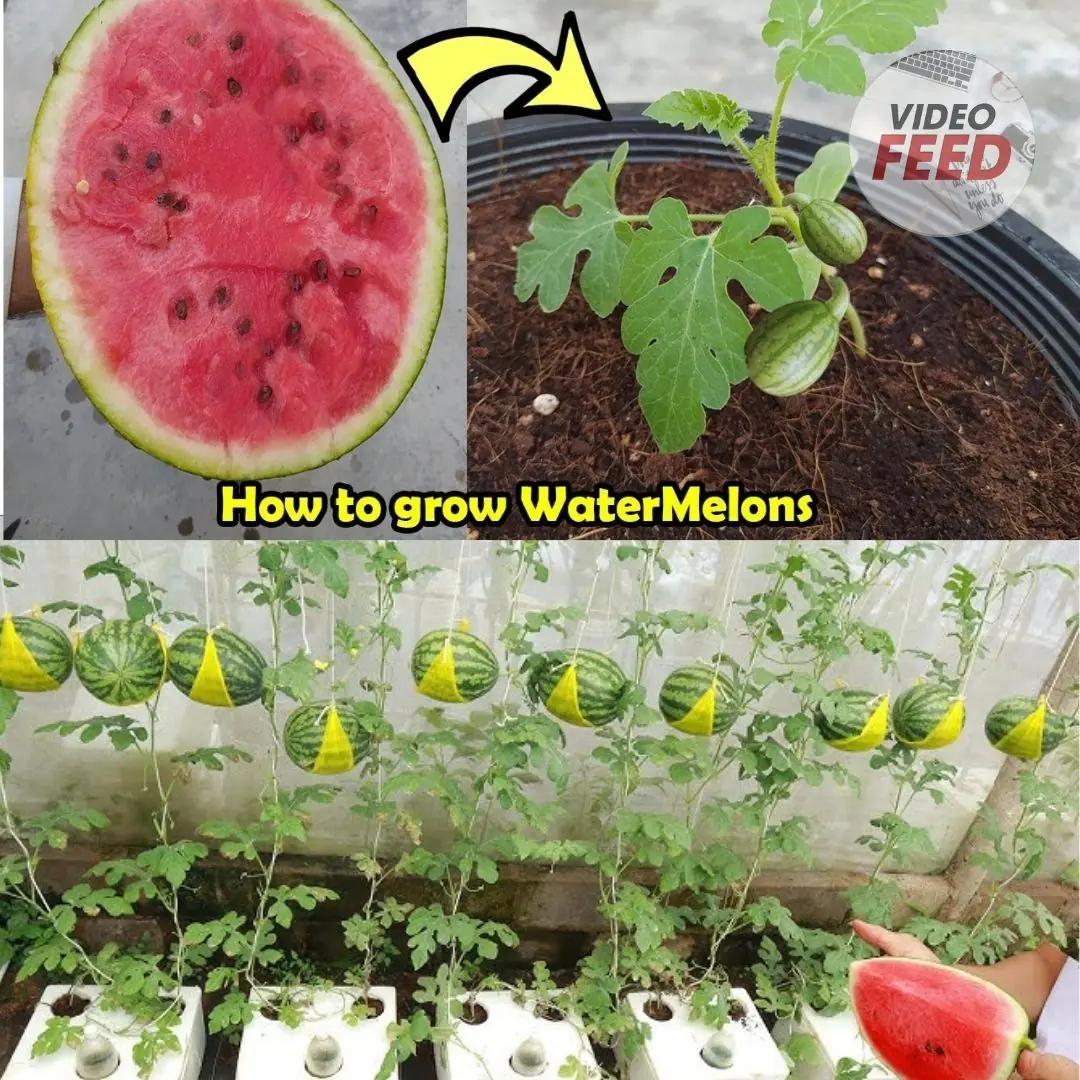
Cantaloupe is typically grown from seeds. Here’s the process for starting your cantaloupe plants:
Timing: Start planting cantaloupe seeds outdoors only when the risk of frost has passed, and the soil temperature is consistently above 70°F (21°C). This usually happens in late spring or early summer.
Spacing: Plant cantaloupe seeds 1 inch (2.5 cm) deep and space them about 18-36 inches (45-90 cm) apart, depending on the variety. Leave at least 3 feet (91 cm) between rows to provide plenty of space for vines to spread.
Transplanting (Optional): If you’re starting cantaloupe indoors, start seeds 2-3 weeks before the last expected frost and transplant seedlings when the outdoor conditions are ideal for growth.
Proper care is key to a successful cantaloupe harvest. Here are some essential tips:
Watering: Keep the soil consistently moist but not soggy. Water the plants deeply to encourage strong root growth, particularly during the flowering and fruiting stages. Avoid overhead watering, as wet leaves can promote fungal diseases.
Mulching: Apply mulch around the base of the plants to retain moisture, suppress weeds, and maintain an even soil temperature.
Fertilization: Use a balanced, slow-release fertilizer rich in phosphorus and potassium to promote strong flowers and fruit development. Avoid excessive nitrogen, as it can lead to vigorous leaf growth at the expense of fruit production.
Pruning: Pruning isn’t strictly necessary, but you can pinch back the vines once they have 4-6 leaves to encourage lateral growth and larger fruits. This also helps the plant focus energy on producing fruit.
Cantaloupe plants produce both male and female flowers. Pollination is crucial for fruit production, and it is typically carried out by bees and other pollinators. If you’re growing cantaloupe in an area with limited pollinator activity, consider hand-pollinating the flowers.
To hand-pollinate:
Use a small brush or cotton swab to transfer pollen from the male flowers (which have thin stems) to the female flowers (which have small fruit buds at the base).
Cantaloupes take about 70-90 days to reach maturity, depending on the variety and growing conditions. Here’s how to know when to harvest:
Color Change: The skin of the cantaloupe should change from green to a yellow or beige color, depending on the variety.
Fragrance: Ripe cantaloupe will emit a sweet, fruity aroma near the stem end.
Slip from the Vine: One of the most telling signs of ripeness is when the melon easily slips off the vine with a gentle tug. The stem should be slightly dry, indicating that the melon is fully ripe.
Sound: When tapped, a ripe cantaloupe will produce a hollow sound.
Once harvested, store cantaloupes in a cool, dry place. Uncut cantaloupes can be stored at room temperature for up to a week, allowing the flavor to develop. Once cut, refrigerate the melon and consume it within a few days.
Growing cantaloupe in your garden can be a fun and rewarding experience, especially when you’re able to enjoy the sweet, juicy fruit you’ve cultivated yourself. By choosing the right variety, preparing the soil, ensuring proper care, and watching for the signs of ripeness, you can successfully grow cantaloupe and harvest your own delicious melons.
Happy gardening and enjoy your homegrown cantaloupes!
5 Health Benefits of Eating Watermelon Seeds



















The White Mulberry Tree: An Overlooked Source of Incredible Health Benefits

Signs in Your Hand Veins That May Be Linked to Kidney Health

Doctors Say Eating Cashews Does THIS to Your Body… Find Out Below

Notice These 8 Morning Bathroom Signs? Get Medical Help Right Away

14 Reasons Avocados Deserve Their Superfood Status
Eat Eggs and Sweet Potatoes Every Morning—Here Are 13 Reasons Why
This small detail could turn $2 into thousands

This daily habit could be helping—or hurting—you

Doctors reveal what visible veins really mean

I thought it was nothing… until I looked closer

You’ve seen this hand gesture a thousand times—but its meaning will surprise you

He thought it was passion—seconds later, it turned into a life-threatening emergency

A Simple Natural Ingredient That May Support Better Sleep and Digestion

This Vietnamese fruit is rich in antioxidants tied to cancer defense.

10 foods that don’t go well with eggs and why you should be careful

Don’t Toss Pumpkin Seeds – They’re a Powerful Hidden Superfood

A simple clove habit may offer surprising daily health benefits.
Waking up with heel pain, even without standing much? Your body may be trying to tell you something important.

Discover 7 Surprising Health Benefits of Chicken Gizzards

Common early symptoms of kidney disease and how to prevent further damage